Addressing Global Reproductive and Sexual Health Needs
Reproductive health concerns all matters pertaining to the physical, emotional, and social well-being relating to the reproductive system. Reproductive health is a right, not a privilege. The predominant global male role in family planning is a passive one, where the majority of reproductive responsibility has been assigned to females. This is reflected by the dominant focus of contraceptive research on females, while men do not have access to any form of reversible, long-acting, effective contraceptives. Because of this, men have lost a significant element of their reproductive autonomy. Simultaneously, there is unequal and inadequate distribution of modern contraceptive methods to rural and impoverished communities resulting in the global population epidemic. My honors project focused on investigating bioactive phytoconstituents with male antifertility and spermicide properties from Azadirachta indica, and Gossypium. My intention was to design a dose-dependent male contraceptive using traditional medicine. I have researched the biochemistry and physiology of the male reproductive system and analyzed how these phytoconstituents interact within the body. To emphasize the importance of this research, I established the current global situation of the increasing world population and inaccessibility of millions to western contraceptive methods. I finally identified institutional factors that influenced male role in family planning and contraceptive use including ethics, patriarchy, cultural and socioeconomic environments, education, and healthcare systems. Ultimately, I proposed some future avenues for research in the development of a male contraceptive.
"Boys should be told that becoming contraceptive responsible extends beyond just wearing the condom. It includes a desire to share the expenses of contraceptives used by the girl, help and support her to decide the best contraceptive, or postpone sexual intercourse when no contraceptive is available. Both need to be educated in contraception and encouraged to support each other’s effort to prevent pregnancy.” (Chng et al 2018).
To improve the sexual and reproductive health of both genders, there needs to be a change in the societal role of men in family planning and safe sex practices. With the widespread prevalence of the female birth control pill and other contraceptive methods, pregnancy prevention efforts are focused on women, often ignoring the role of men in contraceptive use. The result is that women are unfairly burdened with the responsibility of family planning. Females been forced to bear the unequal financial and health-related responsibilities of unplanned pregnancies, while men have lost a significant part of their reproductive autonomy. Globally, young men must be educated and encouraged to become active participants. By having access to their own forms of reversible, effective contraceptives, males simultaneously achieve reproductive autonomy and become active members in family planning.
Azadirachta indica is commonly known as neem. Neem is able to interact with the spermatogenesis process and alter the structure and function of the testes which therefore inhibit the integrity of the spermatozoa and disrupts the normal functioning of the male reproductive system. Neem is found in several regions including Asia, Africa, America, and Australia. It can survive in different conditions such as rocky and dry soil and in various climates. It grows up to 700 meters in height and lives for more than 200 years. Neem has been used for its antifertility properties in both genders across the globe. For instance, women in northwestern Madagascar villages consume neem leaves for their contraceptive use. In Gambia and Ghana, neem leaves are made as a tea drink to prevent pregnancy. These tea drinks are given to people by the first two or three years of their lives. In the 1980s, neem oil was first tested as a male contraceptive in monkeys and found to induce reversible infertility without affecting sperm production or libido. In many rural regions of India, men consume neem extract to achieve the contraceptive effects. The bioactive molecule is azadirachtin which interacts with enzymes involved in spermatogenesis and disrupts the production of functional sperm. Routes of administration include oral and peritoneal injection. Neem has proven to be a long-acting, reversible form of a. contraceptive.
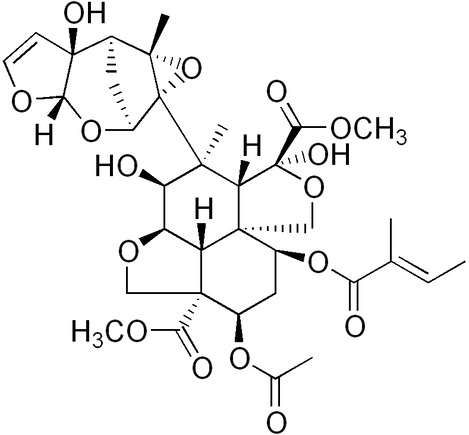
Azadirachtin: Organic Structure of the Bioactive Molecule
Gossypol is a yellowish pigment in cotton plants present in the seeds and root bark. Its antifertility properties were discovered in 1957, when it was reported that between 1930 and 1940, Wang village in Jiangsu, China had no childbirths. This phenomenon corresponded to a switch from soybean oil to cottonseed oil for cooking due to economic reasons. Hubei Provincial Group demonstrated crude cottonseed oil to have antispermatogenic effects in rats and monkeys. Later, other studies proved the bioactive molecule was gossypol. Gossypol induces infertility by disrupting the integrity of the plasma membrane of spermatozoa, which arrests sperm function. In the 1970s, after the reports of male infertility being reported from the Wang village, the world became fascinated with researching the potential of gossypol. China was one of the leaders in human trials and was able to study effective doses for gossypol. There were variations in amounts, but the most common doses reported was a concentration of 60-70 mg of gossypol per day for 35 to 42 days which would gradually decreased motility in spermatozoa. Human trials were performed on over 8,000 people until gossypol was abandoned because 0.75% of the test subjects experienced hypokalemia, or the reduction in serum potassium, as a side effect.
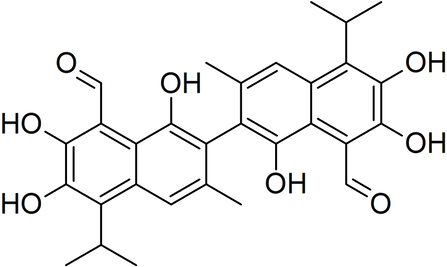
Gossypol: The Organic Structure of the Bioactive Molecule
We already know effective human doses of gossypol. And, because of its nearly 100% efficacy, recent studies have focused on developing methods to modify its metabolism in the body in order to prevent long-term consequences. To address these issues, a male birth control pill with a zero-order release administration is proposed. This means it releases a constant amount of the compound so that the body doesn’t have time to expel it. The means that a small enough amount of the bioactive gossypol would need to be used. Regarding azadirachtin, based on Bansal et al research, the scientists extrapolated that an effective concentration for humans would be a solution containing 10 to 25% of the bioactive azadirachtin (Bansal 2010). Thus, a male birth control pill with a 10-25% mg concentration of azadirachtin and 8.98 to 10.48 either embedded or surrounded by a zero-order gossypol bilayer containing 8.98 to 10.48 mg/kg of active gossypol would prove an effective, relatively safe male contraceptive that would dual-inhibit spermatogenesis and sperm motility.
